Urethroplasty

Urethroplasty
WHAT IS URETHRA?
A tube which carries urine in men and women from the urinary bladder and semen in men from the ejaculatory ducts to the exterior.
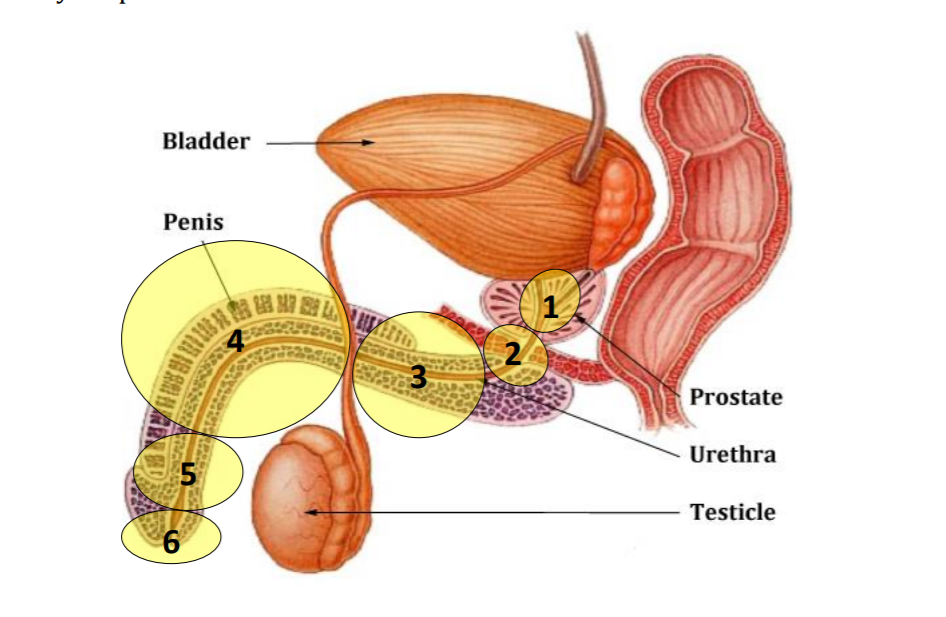
- Prostatic urethra(region 1):The portion passing through prostate.
- Membranous urethra(region 2): The portion passing through your external sphincter (valve) muscle
- Bulbar urethra (region 3): portion passing through the “bulb” of the penis in the perineum
- Penile urethra (region 4): portion passing through the penis
- Sub-meatal urethra or navicular fossa(region 5) : portion passing into the head (glans) of penis
- External meatus (region 6) The visible tip of your urethral opening
- Posterior (rear) urethra (regions 1 - 2)
- Anterior (front) section (regions 3 - 6)
Urologists also describe the urethra as being divided into two main sections:
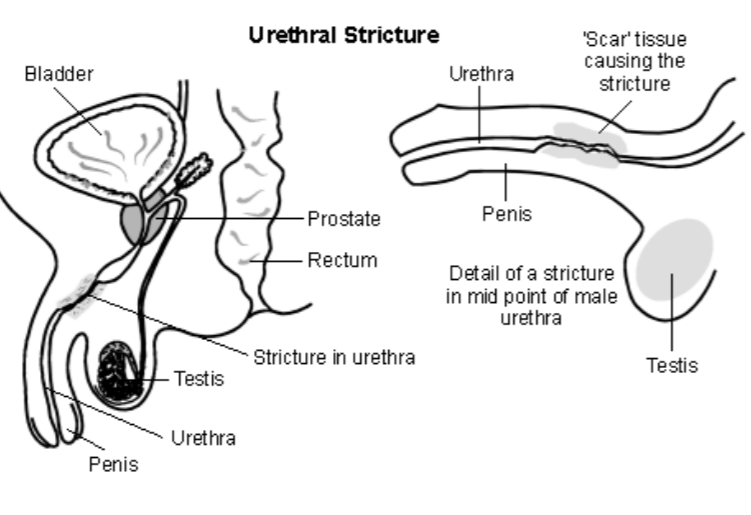
WHAT IS URETHRAL STRICTURE
Urethral stricture is a narrowing of the lumen urethra(the tube conducting urine from the bladder to the exterior) caused by injury, instrumentation or infection . Stricture is more common in men because of a longer length of urethra as compared to women
WHAT ARE THE SIGNS OF URETHRAL STRICTURE
- Weak urine stream.(most common cause of weak stream in men between 20 to 40 years).
- Feeling of incomplete bladder emptying after urination.
- Interrupted urine stream
- Pain or burning during urination.
- Inability to control urination (incontinence)
- In an elderly male symptoms of stricture and prostate enlargement are same. In fact both may exist simultaneously. Sometimes stricture is found incidentally while performing scopy for a prostate surgery and is treated at the same time during prostate surgery.
WHAT ARE THE CAUSES OF STRICTURE?
- Idiopathic :Cause unknown
- Infections especially sexually-transmitted Diseases (STDs) like gonorrhoea
- Inflammation e.g. lichen sclerosus (LS) also known as balanitis xerotica obliterans (BXO)
- Trauma: Caused by injury to the urethra, e.g. a fall astride the cross-bar of a bicycle or a crushing pelvic trauma
- Iatrogenic : Caused by procedures involving instrumentation of the urethra, like prostate surgery
- Urethral catheterisation .
- Radiotherapy or surgery to adjacent organs
- Congenital Inherited conditions like hypospadias (or as a result of previous surgery to correct hypospadias)
- Cancer is a rare cause
HOW IS URETHRAL STRICTURE DIAGNOSED?
It can be diagnosed by a urologist by :
1.Clinical: History and examination(the visible external urinary opening called meatus may appear narrow)
2. Uroflowmetry: A test to see the strength of urine by asking the person to void in a commode connected to a machine called as Uroflowmeter.
3. Urethrogram: A specialized X Ray wherein a dye is passed through the urinary passage and X ray images are taken to delineate the urinary passage.
4. Cystoscopy: An endoscopic direct visualization of urinary passage. A short narrowing can be treated simultaneously during cystoscopy.
5.Many times stricture detected incidentally during failure to insert a urinary catheter during an unrelated surgery or medical condition like need for catheterization for monitoring urine output.
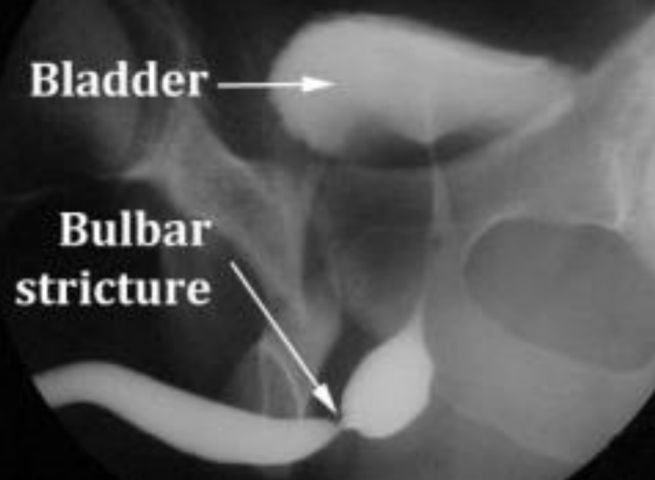
ASCENDING URETHROGRAM SHOWING STRICTURE SITE
ARE THERE ANY PREVENTIVE MEASURES?
Since STDs are one factor, safe sexual practices can reduce chances of stricture formation.
ARE STRICTURES DANGEROUS? WHAT ARE THE RISKS OF AN UNTREATED STRICTURE?
- The urine may stop completely requiring catheter placement directly through the lower tummy in emergency(Supra Pubic Catheterisation).
- Long standing strictures if left untreated, may cause back pressure in kidneys leading to kidney failure.
- It can lead to recurrent or severe urinary infection
- It can lead to stone formation in the urinary bladder
WHAT IS THE TREATMENT FOR STRICTURES
Remember that there is no natural remedy or medicine to treat a stricture
Treatment options include:
- Urethral dilatation.
- Internal urethrotomy.
- Urethral reconstruction.
- Urethral diversion
- Observation
Urethral Dilatation
Under local or general anesthesia, a plastic or metal dilator passed into urethra to stretch the narrow area.
DVIU/OIU( Direct Visual Internal Urethrotomy or Optical Internal Urethrotomy). A urethrotomy is when the cystoscope is used to cut a ring of scar tissue with a small knife to enlarge the area of blockage.
After the procedure, an indwelling catheter is usually left in place for 3 to 5 days. The most common problem of dilatation/urethrotomy is the return of the stricture, which is expected in almost all the cases. You can expect blood in the urine for a period of time after this or uncommonly an episode of urinary infection
URETHROPLASTY
When dilatation/urethrotomy fails and the stricture returns, urethral reconstruction may be needed to try to get more lasting result in terms of creating enough passage through the urethra. These are complex operations,requires a longer anaesthetic time, it is open (cutting) surgery and it has a higher risk of side effects but a higher success than internal optical urethrotomy or urethral dilatation. The type of procedure depends on the site, length and tightness of the strictur
End to End or Anastomotic Urethroplasty: In short strictures of bulbar urethra, the urethra is reconstructed by removing the strictured segment and then suturing the ends of normal urethra back together over a catheter
Substitution Urethroplasty: When stricture length is very long or located in the penile part of the urethra, the urethra may be rebuilt using the lining of the inside of the cheek(Buccal Mucosal Graft Urethroplasty) or skin flaps from the penis or scrotum. Using these methods, the urethra can be reconstructed in most cases with a good long-term success rate.
Urethroplasty
Sometimes staging of the surgery may be required, with two operations several months apart. It is most often used for strictures of the penile urethra.
- In the first stage,a cut is made on the under-surface of penis, the urethra laid open and all diseased tissue removed . A piece of buccal mucosa (cheek lining) is used as a graft and fixed in place with stitches so looks like a quilt. We stitch the skin of the penis back to the edges of the graft, leaving the graft itself exposed. After this, your urethral meatus (external opening) will be further back on the underside of your penis than it was before the procedure. A catheteris left into the bladder for two to three weeks.
- The second stage is performed several months later, once the graft has picked up a new blood supply. The graft is rolled into a tube to reconstruct the urethra, over a catheter into your bladder for two to three weeks.
Single-stage penile urethroplasty
Here, the reconstruction is done as a single operation. We normally use a buccal mucosa graft, but we sometimes use a flap of skin (with its own blood supply) from the shaft of the penis or the foreskin to enlarge the urethra

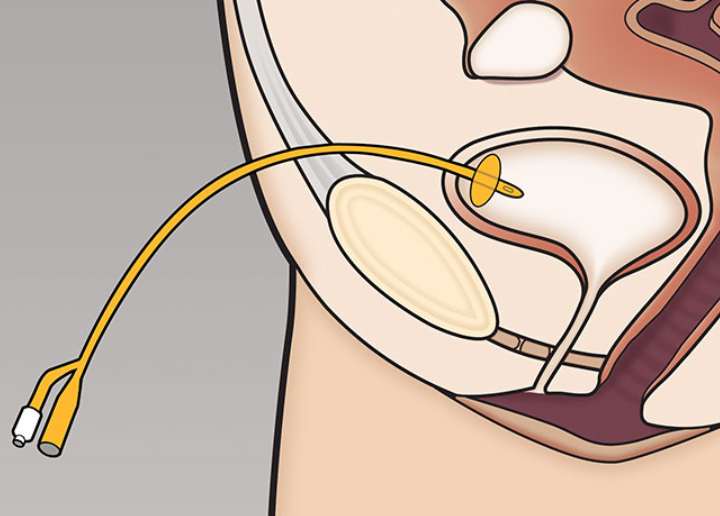
Long-term urethral catheter or suprapubic catheter
Someone with multiple medical problems or someone who does not want an invasive treatment, a long-term catheterthrough the urethra (a urethral catheter) or through the tummy wall above the pubic bone (a suprapubic catheter) may be opted for. Long-term catheters need to be changed every month.
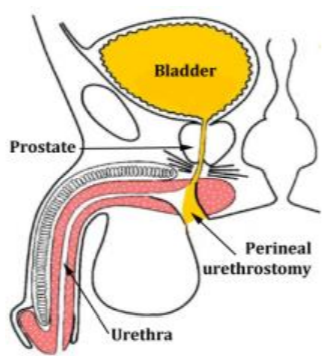
Perineal urethrostomy
This is a procedure to bypass the diseased urethra by bringing out a normal portion of the urethra to the skin surface in the perineum (between the back of the scrotum and the anus, pictured). It is only used if the bulbar urethra is healthy and of normal diameter. It is less complex than urethroplasty, and may be considered if you have extensive stricture disease where reconstructive surgery might not be technically possible, or if you wish to avoid further surgery. It results in urine being passed through an opening in the perineum, rather than along the penis. After this, you will need to sit down to pass urine. You will also ejaculate through this opening (not through your penis.
All the above proceduresneed an incision (cut) in your perineum (between your anus & scrotum), a 1 or 2-day hospital stay, a catheter in your bladder for 2 - 3 weeks and 4 - 6 weeks off work CAN STRICTURE RECUR AFTER SURGERY?
Unfortunately YES!
Recurrence rates after DVIU are almost 90-100 percent
Recurrence rates after urethroplasty vary between 11-30 percent.
To reduce the chances of the urethra to narrow again, sometimes self caliberation is taught to the patient. It means that a person is asked to pass a lubricated tube or catheter on his own on regular intervals (1-3 times in a week) for a few seconds. If a person is unable to do so on his own then it is taught to the caretaker or the patient asked to visit OPD on regular intervals for the same.
A repeat surgery may be required for a recurrence.